Header Image: Kenneth Edward | Biografx | Getty Images
Basic Information
|
Sarin is classified as an organophosphorous compound and is a strong nerve agent. Its IUPAC name is (RS)-Proapn-2-yl methylphophonofluoridate. It is a colorless, odorless, and tasteless liquid that is highly volatile. Because its vapors are almost five times denser than air, they tend to move along surfaces and collect in areas with poor ventilation. It can be absorbed by the body by various means including through the skin. Sarin can also produce hydrofluoric acid at low pH, decompose various metals, and is combustible.
Because sarin is such a potent nerve agent, small amounts are enough to produce fatal results. The skin lethal dose (LD50) for humans is 28 mg/kg. Orally in rats, the LD50 is 550 μg/kg. Since sarin is commonly dispersed as a gas, its lethal concentration (LCt50) in the air is 35 mg-min/m3 for a normally breathing adult. |
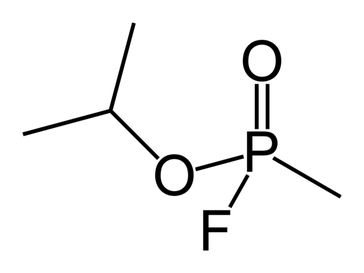
(RS)-Propan-2-yl methylphosphonofluoridate
|
Mechanism
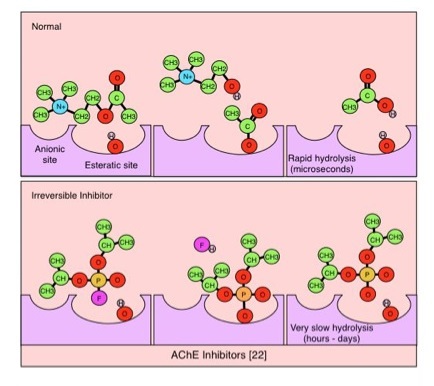 By Sbolmer (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons / Removed middle diagram from original
By Sbolmer (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons / Removed middle diagram from original
Sarin can enter the body by various means including inhalation, ingestion, and absorption through the skin. Once inside the body, sarin acts as an irreversible, highly effective acetylcholinesterase (AChE) inhibitor. In particular, the sarin molecule binds to a serine hydroxyl group in the AChE active site, releasing a fluoride ion. This forms a covalent bond that is stabilized via hydrogen-bond interactions between the oxygens of sarin’s phosphate group and other components of the active site, which makes the binding incredibly stable. Inhibition of this enzyme leads to a decrease in the degradation of acetylcholine (ACh), resulting in increased concentration of ACh in the synapse. Constant synaptic exposure to ACh leads to constant stimulation of the target of the neuron. In the case of sarin, the lethal effects are due to overstimulation of the neuromuscular junction because of the increased concentration of acetylcholine. This overstimulation causes paralysis due to over contraction of muscle cells, which leads to further complications.
Side Effects and Symptoms
|
The primary symptoms of sarin exposure stem from the loss of muscle control due to paralysis from over contraction. This paralysis typically causes death due to loss of essential functions like the respiratory muscles. Because of its potency, death can occur less than ten minutes after initial exposure to a lethal dose. The symptoms tend to follow this general path:
|
|
Treatment
|
Sarin exposure can become fatal very quickly, so treatment must be administered as soon as possible. In general, to treat sarin exposure, one must remove the excess ACh from the synapse in order to ease the overstimulation of the muscles. This is accomplished through the administration of atropine, pralidoxime, and diazepam in combination. Atropine acts as an ACh receptor antagonist by blocking its uptake in the neuromuscular junction by the post-synaptic component, thereby reducing the overstimulation of muscles and the symptoms of sarin exposure (except for the spasms). Diazepam acts as an anticonvulsant by decreasing the release of ACh in order to relieve the spasm symptoms left behind by atropine. Pralidoxime acts as a reactivator to AChE by outcompeting the sarin molecule for the active site of the enzyme, which begins to return the synapse to its normal state.
In cases where these types drugs are not immediately available, physostigmine and mecamylamine can be used quickly to buy some extra time. Mecamylamine acts as a competitive inhibitor of the ACh receptors, blocking the effect of ACh, temporarily imporving symptoms. Physostigmine acts as an inhibitor of AChE, which may seem contradictory. The physostigmine molecules will bind and inhibit AChE, but they are reversible, so they can be taken off the enzyme much more easily than the sarin molecule. Essentially, physostigmine blocks the enzymes from sarin, improving the individuals chances of survival. 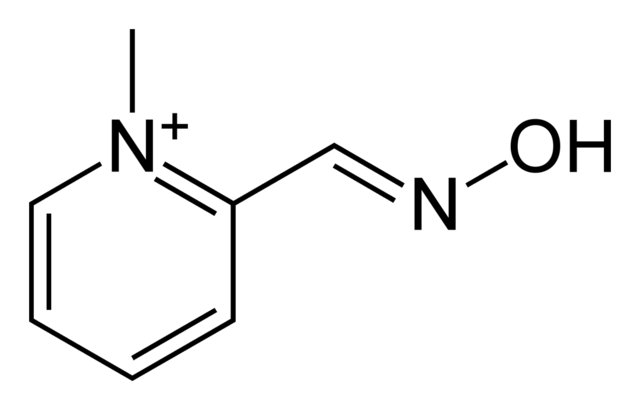
Pralidoxime
|
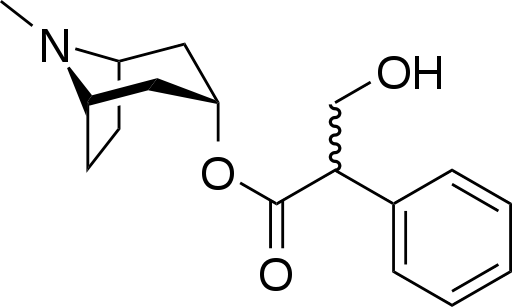
Atropine
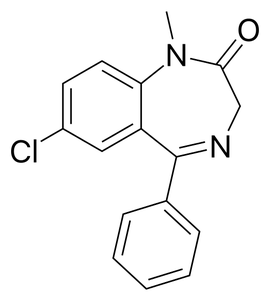
Diazepam
|
