Basic Information
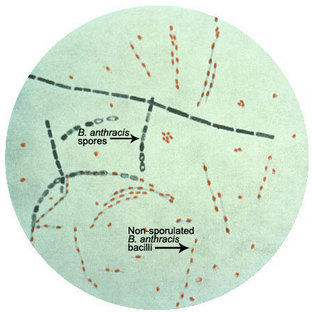
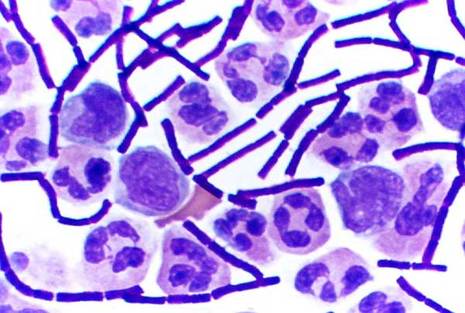
Anthrax is the disease caused by the gram positive, endospore forming, rod-shaped bacterium, Bacillus anthracis. It can grow in an ordinary nutrient medium under aerobic or anaerobic conditions. Spores of B. anthracis occur naturally in the soil and can lay dormant for decades. It most commonly affects domestic and wild herbivores. The spores are nonvirulent, but once a grazing animal ingests it, the spores germinate and switch to their virulent form producing the anthrax toxin, which eventually kills its host. People can contract the disease when they come in contact with infected animals or contaminated animal products. B. anthracis is also one of the most likely agents to be used in a biological attack.
The spores of B. anthracis are light, odorless, and colorless. They are extremely viable even after exposure to extreme temperatures and ultra-violet radiation and they can easily infect a large population quickly and without being detected. This makes them a great biological weapon.
The spores of B. anthracis are light, odorless, and colorless. They are extremely viable even after exposure to extreme temperatures and ultra-violet radiation and they can easily infect a large population quickly and without being detected. This makes them a great biological weapon.
|
|
Mechanism
Once B. anthracis spores germinate in the body of their host they become active and switch from their non-virulent to their virulent form. The major virulence factors of B. anthracis are a poly-D glutamic acid capsule and the anthrax toxin, which is composed of a three-component protein endotoxin.
The poly-D-glutamic acid capsule is composed entirely of poly-D-glutamate. It protects B. anthracis from being recognized and destroyed by the host’s immune system, and allows its unimpeded growth inside the host.
Anthrax toxin is an A/B toxin. The B component is the cell binding component and facilitates edocytosis of the A/B complex. The A component is enzymaticlly active and can affect cell signaling and disrupt normal cell function. Anthrax toxin is composed of:
The mechanism of anthrax toxin entry begins when PA binds a receptor called the anthrax toxin receptor (ATR) present in mammalian cell membranes. Once PA is bound to ATR, a protease from the host cleaves off the N-terminus tail of the PA protein. This induced a switch to PA’s active form. The activated PA binds to six more activated PAs forming a heptamer on the surface of the host cell's membrane. The heptameric complex can then bind either EF or LF. Once PA binds either EF or LF the complex in endocytosed.
Once endocytosed, the environment inside the endosome becomes more acidic and induces a conformational change in the PA heptamer that forms a pore in the endosomal membrane. EF or LF then get injected into the host cell’s cytosol.
EF is a calmodulin-dependent adenylate cyclase. It combines with PA to form the edema toxin of anthrax. EF works similar to the toxins produced by Bordetella pertussis, by activating G-protein signal transduction pathways. This catalyzes the conversion of ATP to cAMP. High levels of intracellular cAMP lead to impaired maintenance of water homeostasis causing cells to swell. In addition, since edema toxin uses ATP to form cAMP, the cell becomes ATP depleted and infected macrophages become bloated and useless since they require ATP in order to engulf and destroy bacteria. This allows the bacteria to further invade the host's immune system.
LF combines with PA to from lethal toxin and cause cell lysis. Lethal factor is a zinc protease that targets members of the mitogen-activated protein kinase kinase (MAPKK) family. Once inside a host cell this protease cleaves MAPKK near their amino terminal end, leading to inhibition of several cell signaling pathways and resulting in an increased amount of cytokines that act as cell mediators. It is believed that high levels of cytokines cause an increase in harmful oxidative molecules inside a cell that eventually causes cell lysis and death.
The poly-D-glutamic acid capsule is composed entirely of poly-D-glutamate. It protects B. anthracis from being recognized and destroyed by the host’s immune system, and allows its unimpeded growth inside the host.
Anthrax toxin is an A/B toxin. The B component is the cell binding component and facilitates edocytosis of the A/B complex. The A component is enzymaticlly active and can affect cell signaling and disrupt normal cell function. Anthrax toxin is composed of:
- PA (Protective antigen)- the B component
- LF (Lethal factor)- the A component
- EF (Edema factor)- the second A component
The mechanism of anthrax toxin entry begins when PA binds a receptor called the anthrax toxin receptor (ATR) present in mammalian cell membranes. Once PA is bound to ATR, a protease from the host cleaves off the N-terminus tail of the PA protein. This induced a switch to PA’s active form. The activated PA binds to six more activated PAs forming a heptamer on the surface of the host cell's membrane. The heptameric complex can then bind either EF or LF. Once PA binds either EF or LF the complex in endocytosed.
Once endocytosed, the environment inside the endosome becomes more acidic and induces a conformational change in the PA heptamer that forms a pore in the endosomal membrane. EF or LF then get injected into the host cell’s cytosol.
EF is a calmodulin-dependent adenylate cyclase. It combines with PA to form the edema toxin of anthrax. EF works similar to the toxins produced by Bordetella pertussis, by activating G-protein signal transduction pathways. This catalyzes the conversion of ATP to cAMP. High levels of intracellular cAMP lead to impaired maintenance of water homeostasis causing cells to swell. In addition, since edema toxin uses ATP to form cAMP, the cell becomes ATP depleted and infected macrophages become bloated and useless since they require ATP in order to engulf and destroy bacteria. This allows the bacteria to further invade the host's immune system.
LF combines with PA to from lethal toxin and cause cell lysis. Lethal factor is a zinc protease that targets members of the mitogen-activated protein kinase kinase (MAPKK) family. Once inside a host cell this protease cleaves MAPKK near their amino terminal end, leading to inhibition of several cell signaling pathways and resulting in an increased amount of cytokines that act as cell mediators. It is believed that high levels of cytokines cause an increase in harmful oxidative molecules inside a cell that eventually causes cell lysis and death.

Symptoms/Adverse Effects
The symptoms of anthrax are dependent on the type of infection. There are four types of anthrax infection.
1. Cutaneous Anthrax
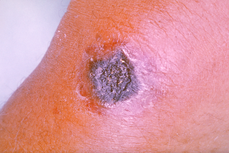
Cutaneous anthrax occurs when anthrax spores enter an open wound in the skin. This normally occurs through cuts or scrapes. This is the most common form of anthrax infection and can happen when a person handles infected animals or contaminated animal products. It affects the skin and tissue around the site of infection.
The infection normally takes one to seven days to develop after exposure. Symptoms include:
1. Cutaneous Anthrax
Cutaneous anthrax occurs when anthrax spores enter an open wound in the skin. This normally occurs through cuts or scrapes. This is the most common form of anthrax infection and can happen when a person handles infected animals or contaminated animal products. It affects the skin and tissue around the site of infection.
The infection normally takes one to seven days to develop after exposure. Symptoms include:
- Swelling around the site of infection
- Small raised bumps that develop into blisters, and later a skin ulcer with a black center
- Swollen lymph nodes
- Headache
- Fever
2. Gastrointestinal Anthrax
Gastrointestinal anthrax normally occurs when a person eats raw or uncooked meat from an animal infected with anthrax. Once ingested the spores can germinate and affect the throat, esophagus, stomach, and intestines. The infection usually takes one to seven days to develop after exposure. Symptoms can include:
Gastrointestinal anthrax normally occurs when a person eats raw or uncooked meat from an animal infected with anthrax. Once ingested the spores can germinate and affect the throat, esophagus, stomach, and intestines. The infection usually takes one to seven days to develop after exposure. Symptoms can include:
- Fever and chills
- Swelling of neck or neck glands
- Sore throat
- Painful swallowing
- Hoarseness
- Nausea and vomiting (especially bloody vomiting)
- Diarrhea or bloody diarrhea
- Headache
- Flushing of the face and red eyes
- Stomach pain
- Fainting
- Swollen abdomen
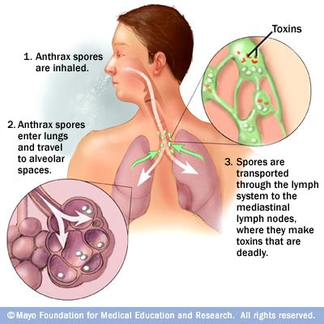
3. Inhalation Anthrax
Inhalation anthrax occurs when a person breathes in anthrax spores. Inhalation anthrax is the most deadly form of anthrax. It is most commonly contracted when workers breathe in airborne anthrax spores while processing infected animal products (such as processing wool or tanning hides). The infection normally develops a week after exposure, but can take up to two months. It starts primarily in the lymph nodes of the chest before spreading to the rest of the body. Symptoms include:
Inhalation anthrax occurs when a person breathes in anthrax spores. Inhalation anthrax is the most deadly form of anthrax. It is most commonly contracted when workers breathe in airborne anthrax spores while processing infected animal products (such as processing wool or tanning hides). The infection normally develops a week after exposure, but can take up to two months. It starts primarily in the lymph nodes of the chest before spreading to the rest of the body. Symptoms include:
- Fever and chills
- Chest discomfort
- Shortness of breath
- Confusion or dizziness
- Cough
- Nausea, vomiting, and stomach pain
- Headache
- Sweats
- Extreme tiredness
- Body Aches

4. Injection Anthrax
Injection anthrax is a new type of anthrax infection that has only been identified in heroin-injecting drug users in northern Europe. Symptoms are similar to that of cutaneous anthrax, but injection anthrax spreads through the body faster and can be harder to recognize and treat. Symptoms include:
Injection anthrax is a new type of anthrax infection that has only been identified in heroin-injecting drug users in northern Europe. Symptoms are similar to that of cutaneous anthrax, but injection anthrax spreads through the body faster and can be harder to recognize and treat. Symptoms include:
- Fever and chills
- Swelling around the site of injection
- Small raised bumps that develop into blisters, and later a skin ulcer with a black center
- Abscesses deep under the skin or in the muscle where the drug was injected
Treatments/Prevention
All types of anthrax can be prevented and treated with antibiotics. Antitoxins as well as vaccines are also available for treatment and prevention of anthrax.
Prevention
Treatment
Prevention
- Antibiotics
- Vaccine
Treatment
- Antibiotics
- Antitoxin

|

|
